Doxycycline Hyclate: Uses, Mechanism, Dosage & Safety Guide
Doxycycline hyclate is a water-soluble, broad-spectrum tetracycline antibiotic used to treat bacterial infections including acne, chlamydia, Lyme disease, and malaria prophylaxis. It also carries significant anti-inflammatory and immunomodulatory properties, making it valuable beyond traditional antibiotic therapy.
What Is Doxycycline Hyclate?
Doxycycline hyclate is a water-soluble form of doxycycline — one of the most widely prescribed tetracycline antibiotics in modern medicine. Unlike some other formulations of doxycycline, the hyclate salt form dissolves readily in water, which contributes to its rapid and nearly complete absorption after oral administration. It is available only with a doctor’s prescription and is used across a broad range of medical specialties, from dermatology and infectious disease to rheumatology and periodontics.
What makes doxycycline hyclate particularly valuable is its dual role in medicine. On one hand, it is a highly effective antibiotic that kills and prevents the growth of a wide range of gram-positive and gram-negative bacteria. On the other hand, it possesses well-documented anti-inflammatory and immunomodulatory effects that make it useful in managing chronic inflammatory conditions that are not traditionally considered infections — such as rosacea, rheumatoid arthritis, and periodontal disease.
In recent years, doxycycline hyclate has also gained attention for its role in postexposure prophylaxis. The Centers for Disease Control and Prevention (CDC) now recommends doxycycline as Doxy PEP — a postexposure prophylaxis strategy where a 200 mg dose is taken within 72 hours after sexual activity to prevent bacterial sexually transmitted infections (STIs) in high-risk populations, including gay, bisexual, and other men who have sex with men, and transgender women with a recent STI history.
FDA-Approved Indications for Doxycycline Hyclate
The Food and Drug Administration has approved doxycycline hyclate for a wide range of bacterial infections and conditions. Understanding the full scope of its approved uses helps both patients and clinicians make informed prescribing decisions.
Sexually Transmitted Infections
Doxycycline hyclate is one of the most commonly prescribed antibiotics for sexually transmitted infections. It is indicated for the treatment of chlamydia (specifically uncomplicated urethral, endocervical, and rectal infections caused by Chlamydia trachomatis), lymphogranuloma venereum, nongonococcal urethritis caused by Ureaplasma urealyticum, and as an alternative agent when penicillin is contraindicated for uncomplicated gonorrhea and syphilis. It is also used in the treatment of pelvic inflammatory disease.
Tick-Borne and Rickettsial Infections
Doxycycline hyclate is a first-line treatment for Rocky Mountain spotted fever, Q fever, tick-borne rickettsial fevers, and relapsing fever caused by Borrelia recurrentis. It is also the preferred antibiotic for Lyme disease — both as prophylaxis following a high-risk Ixodes tick bite (when given within 72 hours of tick removal) and as the preferred oral treatment for erythema migrans, the characteristic skin rash of early Lyme disease.
Respiratory Tract Infections
Doxycycline hyclate is indicated for respiratory tract infections caused by Mycoplasma pneumoniae and Haemophilus influenzae. According to the American Thoracic Society and IDSA guidelines, doxycycline serves as an alternative to macrolides in community-acquired pneumonia for outpatients — particularly when macrolide contraindications such as QT prolongation, drug interactions, or allergy are present.
Skin Conditions
The American Academy of Dermatology recommends doxycycline as the systemic antibiotic of choice for acne vulgaris when systemic therapy is indicated. It is also used as adjunct therapy for severe acne and has demonstrated effectiveness in treating rosacea, bullous dermatoses, granulomatous disease, and livedo vasculitis. For rosacea specifically, a subantimicrobial dose of 40 mg daily works through its anti-inflammatory mechanism rather than its antibiotic action, sparing the body’s healthy microbiome.
Anthrax and Bioterrorism-Related Infections
According to 2023 CDC guidelines, doxycycline hyclate is a first-line agent for both postexposure prophylaxis and treatment of Bacillus anthracis (anthrax) infection in nonpregnant adults without meningitis. It is preferred for uncomplicated cutaneous anthrax and as oral prophylaxis following inhalational anthrax exposure.
Other FDA-Approved Uses
Doxycycline hyclate is also approved for psittacosis caused by Chlamydophila psittaci, inclusion conjunctivitis caused by Chlamydia trachomatis, cholera, tularemia caused by Francisella tularensis, bartonellosis caused by Bartonella bacilliformis, granuloma inguinale, plague caused by Yersinia pestis, brucellosis (in combination with streptomycin), acute intestinal amebiasis, and infections caused by Shigella, Escherichia coli, and Acinetobacter species.
Periodontal Disease
Doxycycline hyclate has a specific approved indication for adult periodontal disease. At subantimicrobial doses of 20 mg twice daily, it acts through its anticollagenase and antimatrix metalloproteinase activity in the gingival crevicular fluid. The American Dental Association recommends this as an adjunct to scaling and root planing in moderate to severe chronic periodontitis.
Mechanism of Action
Understanding how doxycycline hyclate works at the cellular level explains both its broad effectiveness and its unique anti-inflammatory properties.
Antibiotic Action — Inhibiting Bacterial Protein Synthesis
Doxycycline hyclate works primarily through a bacteriostatic mechanism — meaning it stops bacteria from growing rather than directly killing them, though bacterial death ultimately follows. It does this by binding to the 30S prokaryotic ribosomal subunit, which is the machinery bacteria use to build proteins essential for their survival.
More specifically, doxycycline prevents the association of the charged aminoacyl-tRNA (aa-tRNA) with the ribosomal A site, stalling the elongation phase of protein synthesis. The ternary complex — comprised of elongation factor Tu (EF-Tu), GTP, and aa-tRNA — repeatedly attempts to bind the aa-tRNA to the ribosomal A site but fails to do so, creating an unproductive cycle. This halts translation of the growing polypeptide chain, ultimately starving the bacteria of the essential proteins they need to survive and reproduce.
Doxycycline also demonstrates a postantibiotic effect, meaning that bacterial growth remains suppressed even after serum drug concentrations fall below the minimum inhibitory concentration. This contributes to its sustained antimicrobial activity beyond what its blood levels alone would predict.
In terms of how it enters bacteria, doxycycline’s high lipophilicity — compared to other tetracyclines — enables it to cross multiple cellular membranes efficiently. In gram-negative bacteria, it acts as a cationic coordination complex to cross OmpF and OmpC porin channels. In gram-positive bacteria, the electroneutral, lipophilic form traverses the cytoplasmic membrane via an energy-dependent process driven by the proton motive force.
Anti-Inflammatory and Immunomodulatory Action
Beyond its antibiotic properties, doxycycline hyclate inhibits leukocyte movement during inflammation by preventing calcium-dependent microtubular assembly and lymphocytic proliferation. It also initiates anti-inflammatory effects in conditions like osteoarthritis by inhibiting nitric oxide synthase — an enzyme involved in generating the inflammatory molecule nitric oxide. These properties explain its usefulness in treating conditions where inflammation, rather than active infection, is the primary concern.
How Resistance Develops
Bacterial resistance to doxycycline typically develops through ribosomal protection proteins — primarily Tet(O) and Tet(M). These proteins displace doxycycline from its ribosomal binding site and increase the dissociation constant (Kd), allowing normal protein synthesis to resume. Resistance mechanisms also include drug efflux (pumping doxycycline out of the bacterial cell), enzymatic degradation of the drug, and rRNA mutations. Understanding these resistance mechanisms is essential for practicing responsible antimicrobial stewardship.
Pharmacokinetics of Doxycycline Hyclate
Absorption and Bioavailability
Doxycycline hyclate is almost completely absorbed after oral administration, achieving virtually 100% bioavailability — one of the highest of any oral antibiotic. The peak plasma concentration following a 200 mg oral dose in adults is approximately 2.6 µg/mL at 2 hours, decreasing to 1.45 µg/mL at 24 hours. Data shows doxycycline becomes detectable in the blood as quickly as 15 minutes after administration. In children aged 2 to 18 years, absorption is similarly complete, with no meaningful difference between oral and intravenous dosing in terms of systemic exposure.
Distribution
Doxycycline has a volume of distribution of approximately 1.33 L/kg and binds to plasma proteins at about 80% to 90%, which allows for sustained tissue and plasma concentrations. Importantly, the drug crosses the placenta and has been found in fetal tissues — a key reason why it is contraindicated in most pregnancy scenarios.
Metabolism and Elimination
Doxycycline undergoes minimal hepatic metabolism, which is an important advantage over many other antibiotics. It is primarily concentrated in the liver and secreted unchanged in bile, remaining biologically active throughout circulation. In adults with normal renal function, approximately 40% of the drug is excreted unchanged in the urine over 72 hours, with the remainder eliminated through fecal routes. The serum half-life ranges from 18 to 22 hours, which is consistent even in patients with severe renal impairment — making doxycycline one of the few antibiotics that does not require dose adjustment in kidney disease. Hemodialysis does not significantly alter its half-life.
Dosage and Administration
Adult Dosage
For mild to moderate bacterial infections, the standard adult dosage is 100 mg every 12 hours on the first day, followed by 100 mg once daily thereafter. For pelvic infections, 100 mg twice daily for one week is recommended. The maximum dosage is 300 mg/day for most conditions, though acute gonorrheal infections may be treated with up to 600 mg/day for 5 days.
For malaria prophylaxis, 100 mg once daily is taken starting 1 to 2 days before traveling to a high-risk area, continued throughout the trip, and for 4 weeks after returning. For anti-inflammatory purposes — such as in rosacea or periodontal disease — a subantimicrobial dose of 40 mg daily may be used, at which point the drug’s antibiotic mechanism is not activated.
How to Take Doxycycline Hyclate
Doxycycline hyclate is best taken on an empty stomach, at least 1 hour before or 2 hours after eating, with at least 8 ounces of water. Patients should remain upright for at least 30 minutes after taking it to prevent esophageal irritation. For optimal absorption, the medication should be taken 2 to 3 hours before or after consuming any supplements or drugs containing magnesium, zinc, calcium, aluminum, iron, or sodium bicarbonate, as these can significantly reduce absorption.
Available Dosage Forms
Doxycycline hyclate is available in oral capsules (50 mg and 100 mg), oral tablets (20 mg, 50 mg, 75 mg, 100 mg, and 150 mg), delayed-release tablets (50 mg, 60 mg, 75 mg, 80 mg, 100 mg, 150 mg, and 200 mg), and a 100 mg intravenous reconstituted solution for patients unable to take oral medication.
Dosage in Special Populations
In patients with hepatic impairment, no dose adjustment is generally required since doxycycline undergoes minimal hepatic metabolism. However, clinicians should monitor for rare but documented doxycycline-induced liver injury, which can present with a mixed hepatocellular-cholestatic pattern or in association with DRESS syndrome.
In patients with renal impairment, no significant change in the serum half-life is observed, and no dose adjustment is needed. Clinicians should remain aware that tetracyclines carry an antianabolic effect that may increase blood urea nitrogen (BUN) levels.
In older adults, no specific dose adjustments are required, but medication reconciliation is essential due to the increased risk of polypharmacy in this population.
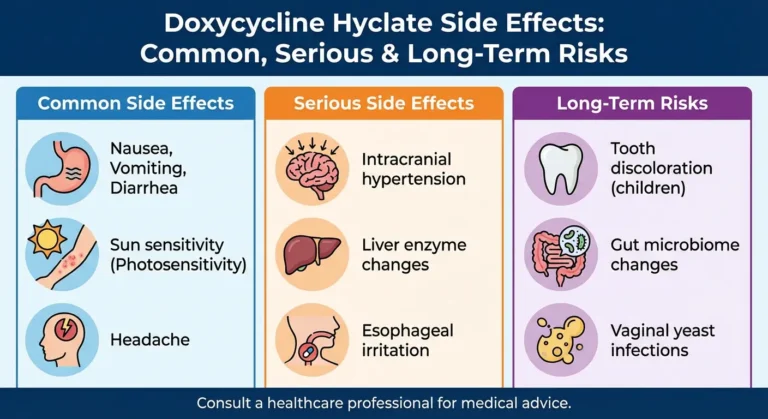
In pediatric patients, doxycycline is contraindicated for nearly all indications in children younger than 8 years, due to the risk of permanent tooth discoloration and suppression of bone growth. Exceptions are made for life-threatening conditions such as anthrax and Rocky Mountain spotted fever when no appropriate alternatives are available.
During pregnancy, doxycycline is associated with retardation of skeletal development and evidence of embryotoxicity. It crosses the placenta and is present in fetal tissues. It is generally contraindicated unless the benefit clearly outweighs the risk.
During breastfeeding, available evidence suggests short-term maternal use carries minimal risk due to low drug concentrations in milk and reduced oral absorption in the infant through calcium binding. However, prolonged or repeated courses should be avoided due to theoretical risks of dental discoloration, bone growth effects, and alteration of the infant’s gastrointestinal flora.
Adverse Effects
Common Side Effects
The most frequently reported adverse effects of doxycycline hyclate include nausea, vomiting, mild diarrhea, photosensitivity (exaggerated sunburn reactions), skin rash or itching, headaches, tooth discoloration, and fixed drug eruption. Most of these are mild and manageable, and many can be reduced by taking the medication with food and plenty of water.
Photosensitivity deserves particular attention. Doxycycline can cause exaggerated sunburn reactions even with brief sun exposure. Patients should minimize sun exposure, wear protective clothing and SPF 30+ sunscreen daily, and avoid tanning beds. Treatment should be discontinued at the first sign of significant skin erythema.
Serious Adverse Effects
Although doxycycline hyclate is generally well tolerated compared to other tetracyclines, serious adverse effects can occur in rare cases. These include hematochezia, leukopenia, hemolytic anemia, esophagitis and esophageal ulcerations (particularly if taken without sufficient water), intracranial hypertension (pseudotumor cerebri), and exacerbation of systemic lupus erythematosus.
In rare cases, doxycycline hyclate has caused Stevens-Johnson syndrome — a potentially life-threatening mucocutaneous eruption with purpuric macules or targetoid lesions requiring hospitalization and supportive care. Other severe cutaneous adverse reactions including toxic epidermal necrolysis, exfoliative dermatitis, erythema multiforme, and DRESS syndrome have also been reported. Doxycycline should be discontinued immediately if any severe skin reactions occur.
Idiopathic intracranial hypertension is a concern particularly in women of childbearing age who are overweight or have a history of this condition. Symptoms include severe headache, visual disturbances, and papilledema. Immediate ophthalmologic evaluation is required if these symptoms develop.
Clostridioides difficile-associated diarrhea (CDAD) can occur during or after doxycycline therapy, ranging from mild diarrhea to fatal colitis. This should be considered in any patient presenting with diarrhea during antibiotic treatment.
Drug Interactions
Several important drug interactions must be considered when prescribing or taking doxycycline hyclate.
Doxycycline can chelate divalent and trivalent cations found in antacids containing aluminum, calcium, and magnesium, as well as oral iron supplements and antidiarrheal agents containing bismuth subsalicylate. This chelation significantly reduces doxycycline absorption, so simultaneous administration should be avoided.
When taken with warfarin, doxycycline can enhance the anticoagulant effect through competitive interaction for albumin binding and potential inhibition of the cytochrome P-450 pathway. Patients on blood thinners require close monitoring when starting or stopping doxycycline.
Barbiturates, carbamazepine, and phenytoin can decrease the serum half-life of doxycycline, potentially reducing its effectiveness. According to product labeling, doxycycline may also reduce the effectiveness of oral contraceptives, so patients should use a backup non-hormonal birth control method during treatment.
The concurrent use of doxycycline and isotretinoin significantly increases the risk of pseudotumor cerebri (idiopathic intracranial hypertension). A drug-free interval of approximately 7 days is recommended between the two medications to allow sufficient washout and minimize overlapping exposure. This combination should be avoided whenever possible.
Other medications associated with photosensitive reactions — including nalidixic acid, amiodarone, voriconazole, hydrochlorothiazide, and thioridazine — may compound the phototoxic effects of doxycycline when used together. Similarly, aminolevulinic acid used in photodynamic therapy can increase light sensitivity and raise the risk of phototoxic reactions.
Contraindications
The absolute contraindication to doxycycline hyclate is a known allergy to doxycycline or any other tetracycline antibiotic. Relative contraindications include liver disease due to rare but documented fatal hepatotoxicity, pregnancy and breastfeeding, concurrent use with penicillin or isotretinoin, a history of fungal infections, recent antibiotic-associated colitis, Clostridioides difficile-associated diarrhea, a history of lupus, porphyria, and in rare cases, myasthenia gravis.
Monitoring
No standard routine tests are required to monitor doxycycline use in short-term therapy. However, for long-term administration, monitoring of phototoxicity, hepatotoxicity through liver function tests (LFTs), and nephrotoxicity is recommended. A complete blood count and peripheral smear monitoring are essential to assess the response to therapy.
For Doxy PEP specifically, guidelines recommend tracking antimicrobial resistance patterns, particularly concerning tetracycline-resistant Neisseria gonorrhoeae and the potential for coselection of beta-lactam resistance.
In the rare event of overdose or hepatic toxicity — which can present 1 to 2 weeks after starting therapy with elevated ALT, AST, alkaline phosphatase, and GGT levels — management focuses on stopping doxycycline immediately. Liver function typically improves within weeks after discontinuation, although severe cholestatic injury may take 2 to 6 months to resolve. Reexposure to doxycycline should be avoided, and caution is advised with other tetracyclines such as minocycline due to potential cross-reactivity.
The Role of Antimicrobial Stewardship
With the expanding clinical uses of doxycycline hyclate and rising concerns about antimicrobial resistance, responsible prescribing has never been more important. Antimicrobial stewardship emphasizes avoiding doxycycline use without confirmed susceptible bacterial strains or a clear prophylactic indication. Clinicians, pharmacists, nurses, and infectious disease specialists all play key roles in ensuring that doxycycline is prescribed, monitored, and used appropriately.
Particularly with Doxy PEP, ongoing surveillance is critical. Concerns about increasing prevalence of tetracycline-resistant Neisseria gonorrhoeae and its potential to coselect for beta-lactam resistance in a first-line treatment target underscore the need for coordinated interprofessional strategies and regular resistance monitoring as this prophylactic use becomes more widespread.
FAQs
What is doxycycline hyclate used for?
Doxycycline hyclate is used to treat a wide range of bacterial infections including acne, chlamydia, syphilis, gonorrhea, Lyme disease, Rocky Mountain spotted fever, community-acquired pneumonia, and anthrax. It is also used for malaria prophylaxis, Doxy PEP for STI prevention, and at sub-antibiotic doses for rosacea and periodontal disease.
What is the difference between doxycycline and doxycycline hyclate?
Doxycycline hyclate is a specific salt form of doxycycline that is water-soluble, which contributes to its high oral bioavailability of nearly 100%. Doxycycline monohydrate is another common salt form that is less water-soluble and is often considered gentler on the stomach. Both contain the same active antibiotic compound and work through the same mechanism.
Does doxycycline hyclate require dose adjustment in kidney disease?
No. Unlike many other antibiotics, doxycycline hyclate does not require dose adjustment in renal impairment because its serum half-life remains consistent at 18 to 22 hours regardless of kidney function. Hemodialysis also does not significantly alter its elimination.
Can doxycycline hyclate be taken with food?
Most formulations of doxycycline hyclate can be taken with food or milk to reduce stomach upset. However, for optimal antibiotic absorption, it is best taken on an empty stomach with a full glass of water. Certain formulations like Oracea must be taken on an empty stomach. Always follow the instructions on your specific prescription.
Is doxycycline hyclate safe during pregnancy?
Doxycycline hyclate is generally not recommended during pregnancy. It crosses the placenta and is associated with retardation of skeletal development and embryotoxicity in animal studies. Taking it in the second half of pregnancy can cause permanent tooth discoloration in the baby. A doctor may only recommend it if the benefit clearly outweighs the risk, such as in a life-threatening infection.
What drugs should not be taken with doxycycline hyclate?
Key interactions to avoid include antacids containing aluminum, calcium, or magnesium (reduce absorption), iron supplements (reduce absorption), warfarin (enhanced anticoagulant effect), isotretinoin (increased risk of intracranial hypertension), and barbiturates or anticonvulsants like carbamazepine and phenytoin (reduce doxycycline half-life).
Final Thoughts
Doxycycline hyclate stands out as one of the most clinically versatile antibiotics available today. Its nearly complete oral bioavailability, consistent pharmacokinetics across diverse patient populations, broad antimicrobial spectrum, and unique anti-inflammatory properties make it a go-to choice across many medical specialties. From treating chlamydia and Lyme disease to preventing malaria and managing rosacea, its range of applications continues to expand — most recently with CDC endorsement as Doxy PEP for STI prevention in high-risk populations.
That said, its power comes with responsibility. Rising resistance — particularly in Neisseria gonorrhoeae and Group A Streptococcus — and the critical importance of appropriate prescribing remind us that doxycycline hyclate should always be used with a clear clinical indication, at the correct dose, for the right duration, and with proper monitoring in place. Used responsibly and within evidence-based guidelines, doxycycline hyclate remains one of modern medicine’s most valuable and reliable antibiotic tools.
Medical Disclaimer: This article is for informational and educational purposes only. It does not constitute medical advice, diagnosis, or treatment recommendations. Always consult a qualified healthcare professional before starting, stopping, or changing any medication. Visit https://doxycycline.blog/ for more information.